Tricuspid Regurgitation (TR) is a complex disease that has multiple causes, and is associated with high rates of morbidity and mortality.1,2 TR is highly prevalent, and among valve diseases, is one of the most undertreated.1,3 If left untreated, TR initiates a cascade of events that can lead to right-sided Heart Failure (HF) and death.4
Summary of current relevant international guidelines on the diagnosis of TR
Transcatheter tricuspid valve intervention has now been elevated to a Class IIa, Level of Evidence (LoE) A recommendation—recognizing its growing role in improving quality of life and promoting right ventricular remodeling. This update reflects a broader commitment to comprehensive, patient-centric care in valvular heart disease and opens new pathways for optimized treatment strategies.
LEARN MORE:
- TR should be evaluated first by echocardiography. In primary TR, specific abnormalities of the valve can be identified. In secondary TR, annular dilatation, along with RV and RA dimensions, as well as RV function should be measured, owing to their prognostic relevance.
- In experienced laboratories, RV strain and/or 3D measurements of RV volumes may be considered to overcome the existing limitations of conventional RV function indices. When available, CMR is the preferred method to assess the RV due to its high accuracy and reproducibility.
- Echocardiographic criteria for grading severity of TR:
- Qualitative: tricuspid valve morphology, color flow regurgitant jet
- Semiquantitative: vena contracta width, proximal isovelocity surface area (PISA) radius, hepatic vein flow, tricuspid inflow
- Quantitative: Effective regurgitant orifice area (EROA), regurgitant volume, enlargement of cardiac chambers/vessels
- In patients with TR, TTE is indicated to:
- evaluate the presence and severity of TR
- determine the etiology
- measure the sizes of the right-sided chambers and inferior vena cava
- assess RV systolic function
- estimate pulmonary artery systolic pressure
- characterize any associated LSHD.
Summary of current relevant international guidelines on the medical management of TR
- In patients with HF, VHD should be managed in a multidisciplinary manner in accordance with clinical practice guidelines for VHD to prevent worsening of HF and adverse clinical outcomes.
- Diuretics are useful in the presence of right HF.
- The addition of an aldosterone antagonist may be considered to counterbalance the activation of the renin-angiotensin-aldosterone system associated with hepatic congestion.
- Dedicated treatment of pulmonary HT is indicated in specific cases.
- Although data are limited, rhythm control may help to decrease TR and contain annular dilatation in patients with chronic AF.
- In the absence of advanced RV dysfunction or severe pulmonary hypertension, none of the above-mentioned therapies should delay referral for surgery or transcatheter therapy.
- The management of HF with TR includes medical therapy (i.e. diuretics, neurohormonal antagonists).
- In patients with signs and symptoms of right-sided HF attributable to severe TR (Stages C and D), diuretics can be useful (Class 2a, Level of evidence C expert opinion).
- In patients with signs and symptoms of right-sided HF attributable to severe secondary TR (Stages C and D), therapies to treat the primary cause of HF (e.g. pulmonary vasodilators to reduce elevated pulmonary artery pressures, guideline-directed medical therapy (GDMT) for HF with reduced LVEF, or rhythm control of AF) can be useful (Class 2a, Level of evidence C expert opinion).
Summary of current relevant international guidelines for surgical management of TR
- Relevant TR requires early intervention to avoid secondary damage of the RV.
- TR should be liberally treated at the time of left-sided valve surgery. Isolated surgery of severe secondary TR (with or without previous left-sided valve surgery) requires comprehensive assessment of the underlying disease, pulmonary hemodynamics, and RV function.
- Primary TR:
- Surgery is recommended in patients with severe primary TR undergoing left-sided valve surgery (Class I, Level of evidence C)
- Surgery is recommended in symptomatic patients with isolated severe primary TR without severe RV dysfunction (Class I, Level of evidence C)
- Surgery should be considered in patients with moderate primary TR undergoing left-sided valve surgery (Class IIa, Level of evidence C)
- Surgery should be considered in asymptomatic or mildly symptomatic patients with isolated severe primary TR and RV dilatation who are appropriate for surgery (Class IIa, Level of evidence C)
- Secondary TR:
- Surgery is recommended in patients with severe secondary TR undergoing left-sided valve surgery (Class I, Level of evidence B)
- Surgery should be considered in patients with mild or moderate secondary TR with a dilated annulus (≥40 mm or >21 mm/m2 by 2D echocardiography) undergoing left-sided valve surgery (Class IA, Level of evidence B)
- Surgery should be considered in patients with severe secondary TR (with or without previous left-sided surgery) who are symptomatic or have RV dilatation, in the absence of severe RV or left ventricular dysfunction and severe pulmonary vascular disease/hypertension (Class IIa, Level of evidence B).
- Transcatheter therapy and surgery may be considered in selected cases. A multidisciplinary heart team, including HF specialists, should be considered for assessment and treatment planning.
- Transcatheter techniques have recently emerged as potential treatment options of TR. Preliminary results show improvement in TR severity and symptoms with low complication rates. Further prospective studies are needed to show the prognostic impact of these treatments in HF patients
- Consider surgical tricuspid valve repair at the time of MV surgery when TR is moderate or severe.
- Consider surgical tricuspid valve repair at the time of aortic valve surgery when TR is severe.
- For patients with VHD for whom intervention is contemplated, individual risks should be calculated for specific surgical and/or transcatheter procedures, using on-line tools when available, and discussed before the procedure as a part of a shared decision-making process (Class 1, Level of evidence C expert opinion).
- Patients with severe VHD should be evaluated by a multidisciplinary heart valve team when intervention is considered (Class 1, Level of evidence C expert opinion).
- In asymptomatic patients with any type of valve intervention, a baseline postprocedural TTE followed by periodic monitoring with TTE is recommended.
- In patients with severe TR (Stages C and D) undergoing left-sided valve surgery, tricuspid valve surgery is recommended (Class 1, Level of evidence C limited data).
Summary of current relevant international guidelines for surgical management of TR
- Transcatheter tricuspid valve intervention TTVIs are under clinical development and early registry and study data have demonstrated their feasibility to reduce TR.
- Transcatheter treatment of symptomatic secondary severe TR may be considered in inoperable patients at a heart valve center with expertise in the treatment of tricuspid valve disease (Class IIb, Level of evidence C).
- Transcatheter therapy and surgery may be considered in selected cases. A multidisciplinary heart team, including HF specialists, should be considered for assessment and treatment planning.
- Transcatheter techniques have recently emerged as potential treatment options of TR. Preliminary results show improvement in TR severity and symptoms with low complication rates. Further prospective studies are needed to show the prognostic impact of these treatments in HF patients
- For patients with VHD for whom intervention is contemplated, individual risks should be calculated for specific surgical and/or transcatheter procedures, using on-line tools when available, and discussed before the procedure as a part of a shared decision-making process (Class 1, Level of evidence C expert opinion).
Clinical case clubs | Educational tools | Hot topics
Expert opinions | Live & online discussions
TV

TAVI in complex anatomies

AI-enabled procedural learning

Case planning for lifetime management

Strategies to reduce conduction disturbances following TAVI

TAVI Summit 2026 - Introduction

EuroPCR 2026 Symposium

Artifical intelligence in structural heart imaging

Anatomy for structural heart therapies

EACTS Symposium 2025
Transcatheter Aortic Valves Implant - 2025
HUB
Tri.Fr 2 years outcomes
bRIGHT clinical data release | PCR LV 2025
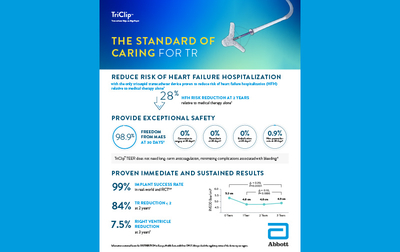
The standard of caring for TR

TEER G5 Brochure 2025
TRILUMINATE Pivotal - 2-year update EuroPCR 25
bRIGHT 2-year real-world outcomes
2-year outcomes from the TRILUMINATE Pivotal trial

bRIGHT study
- Falk V, Baumgartner H, Bax JJ et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur J Cardiothorac Surg. 2017;52(4):616–664. doi.org/10.1093/ejcts/ezx324.
- Lindroos M, Kupari M, Heikkilä J et al. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol. 1993;21(5):1220–1225. doi.org/10.1016/0735-1097(93)90249-Z.
- Osnabrugge RLJ, Mylotte D, Head SJ et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. 2013;62(11):1002–1012. doi.org/10.1016/j.jacc.2013.05.015.
- d'Arcy JL, Coffey S, Loudon MA et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur Heart J. 2016;37(47):3515–3522. doi.org/10.1093/eurheartj/ehw229.
- van Geldrop MWA, Heuvelman HJ, Kappetein AP et al. Quality of life among patients with severe aortic stenosis. Neth Heart J. 2013;21(1):21–27. doi.org/10.1007/s12471-012-0364-9.
- Oterhals K, Haaverstad R, Nordrehaug JE et al. Self-reported health status, treatment decision and survival in asymptomatic and symptomatic patients with aortic stenosis in a Western Norway population undergoing conservative treatment: a cross-sectional study with 18 months follow-up. BMJ Open. 2017;7(8):e016489. dx.doi.org/10.1136/bmjopen-2017-016489.
- Iung B, Baron G, Tornos P et al. Valvular heart disease in the community: a European experience. Curr Probl Cardiol. 2007;32(11):609–661. doi.org/10.1016/j.cpcardiol.2007.07.002.
- Faggiano P, Frattini S, Zilioli V et al. Prevalence of comorbidities and associated cardiac diseases in patients with valve aortic stenosis. Potential implications for the decision-making process. Int J Cardiol. 2012;159(2):94–99. doi.org/10.1016/j.ijcard.2011.02.026.
- Maisano F, Worthley S, Rodés-Cabau J et al. Early commercial experience from transcatheter aortic valve implantation using the Portico™ bioprosthetic valve: 30-day outcomes in the multicentre PORTICO-1 study. EuroIntervention. 2018;14(8):886–893. doi.org/10.4244/EIJ-D-18-00343.
- Reardon MJ, Van Mieghem NM, Popma JJ et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376(14):1321–1331. doi.org/10.1056/NEJMoa1700456.
- Leon MB, Smith CR, Mack MJ et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374(17):1609–1620. doi.org/10.1056/NEJMoa1514616.
- Olszowska M. Pathogenesis and pathophysiology of aortic valve stenosis in adults. Pol Arch Med Wewn. 2011;121(11):409–413. www.mp.pl/paim/issue/article/1103/.
- Czarny MJ et al. Diagnosis and management of valvular aortic stenosis. Clin Med Insights Cardiol. 2014;8(Suppl 1):15–24. doi.org/10.4137/CMC.S15716.
- Nishimura RA, Otto CM, Bonow RO et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. 2014;148(1):e1–e132. doi.org/10.1016/j.jtcvs.2014.05.014.
- Zakkar M, Bryan AJ, Angelini GD. Aortic stenosis: diagnosis and management. BMJ. 2016;355:i5425. doi.org/10.1136/bmj.i5425.
- Indolfi C, Bartorelli AL, Berti S et al. Updated clinical indications for transcatheter aortic valve implantation in patients with severe aortic stenosis: expert opinion of the Italian Society of Cardiology and GISE. J Cardiovasc Med (Hagerstown). 2018;19(5):197–210. doi.org/10.2459/JCM.0000000000000636.
- Grimard BH, Safford RE, Burns EL. Aortic stenosis: diagnosis and treatment. Am Fam Physician. 2016;93(5):371–378. www.aafp.org/pubs/afp/issues/2016/0301/p371.html.
- Vahanian A, Beyersdorf F, Praz F et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. doi.org/10.1093/eurheartj/ehab395
- Kanwar A, Thaden JJ, Nkomo VT. Management of patients with aortic valve stenosis. Mayo Clin Proc. 2018;93(4):488-508. doi.org/10.1016/j.mayocp.2018.01.020.
- “Aortic Valve Stenosis - Diagnosis and Treatment - Mayo Clinic.” Aortic Valve Stenosis - Diagnosis and Treatment - Mayo Clinic, 18 August 2022, www.mayoclinic.org/diseases-conditions/aortic-stenosis/diagnosis-treatment/drc-20353145 (accessed May 2023).
- Ram E, Sternik L, Lipey A, et al. Clinical and echocardiographic outcomes after aortic valve repair in patients with bicuspid or unicuspid aortic valve. Isr Med Assoc J. 2018;20(7):423–428. www.ima.org.il/FilesUploadPublic/IMAJ/0/294/147319.pdf.
- Martín M, Lorca R, Rozado J, et al. Bicuspid aortic valve syndrome: a multidisciplinary approach for a complex entity. J Thoracic Dis. 2017;9(Suppl 6):S454–S464. doi.org/10.21037/jtd.2017.05.11.
- Généreux P, Stone GW, O'Gara PT et al. Natural history, diagnostic approaches, and therapeutic strategies for patients with asymptomatic severe aortic stenosis. J Am Coll Cardiol. 2016;67(19):2263–2288. doi.org/10.1016/j.jacc.2016.02.057.
- Lund O. Preoperative risk evaluation and stratification of long-term survival after valve replacement for aortic stenosis. Reasons for earlier operative intervention. Circulation. 1990;82(1):124–139. doi.org/10.1161/01.CIR.82.1.124.
- Nashef SA, Roques F, Sharples LD et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734–744;discussion 744–745. doi.org/10.1093/ejcts/ezs043.
- Roques F, Michel P, Goldstone AR et al. The logistic EuroSCORE. Eur Heart J. 2003;24(9):881–882. doi.org/10.1016/S0195-668X(02)00799-6.
- Roques F, Nashef SA, Michel P et al. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg. 1999;15(6):816–822;discussion 822–823. doi.org/10.1016/S1010-7940(99)00106-2.
- Thourani VH, Suri RM, Gunter RL et al. Contemporary real-world outcomes of surgical aortic valve replacement in 141,905 low-risk, intermediate-risk, and high-risk patients. Ann Thorac Surg. 2015;99(1):55–61. doi.org/10.1016/j.athoracsur.2014.06.050.
- Brown JM, O’Brien SM, Wu C et al. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg. 2009;137(1):82–90. doi.org/10.1016/j.jtcvs.2008.08.015.
- Culler SD, Cohen DJ, Brown PP et al. Trends in aortic valve replacement procedures between 2009 and 2015: has transcatheter aortic valve replacement made a difference? Ann Thorac Surg. 2018;105(4):1137–1143. doi.org/10.1016/j.athoracsur.2017.10.057.
- O'Brien SM, Shahian DM, Filardo G et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2--isolated valve surgery. Ann Thorac Surg. 2009; 88(1 Suppl):S23–42. doi.org/10.1016/j.athoracsur.2009.05.056.
- Durko AP, Osnabrugge RL, Kappetein AP. Long-term outlook for transcatheter aortic valve replacement. Trends Cardiovasc Med. 2018;28(3):174–183. doi.org/10.1016/j.tcm.2017.08.004.
- McDonagh TA, Metra M, Adamo M et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi.org/10.1093/eurheartj/ehab368.
- Filardo G, Hamilton C, Hamman B et al. New-onset postoperative atrial fibrillation and long-term survival after aortic valve replacement surgery. Ann Thorac Surg. 2010;90(2):474–479. doi.org/10.1016/j.athoracsur.2010.02.081.
- European Heart Journal, Volume 46, Issue 44, 21 November 2025, Pages 4635–4736, doi.org/10.1093/eurheartj/ehaf194