Trikuspidalinsuffizienz (TI) ist eine komplexe Krankheit, die mehrere Ursachen hat und mit hohen Morbiditäts- und Mortalitätsraten verbunden ist.1,2 TI ist weit verbreitet und zählt unter den Klappenerkrankungen zu den am wenigsten behandelten Erkrankungen.1 Unbehandelt löst die TI eine Kaskade von Ereignissen aus, die zu rechtsseitiger Herzinsuffizienz (HI) und zum Tod führen können.4
Transcatheter tricuspid valve intervention has now been elevated to a Class IIa, Level of Evidence (LoE) A recommendation—recognizing its growing role in improving quality of life and promoting right ventricular remodeling. This update reflects a broader commitment to comprehensive, patient-centric care in valvular heart disease and opens new pathways for optimized treatment strategies.
LEARN MORE:
- TR should be evaluated first by echocardiography. In primary TR, specific abnormalities of the valve can be identified. In secondary TR, annular dilatation, along with RV and RA dimensions, as well as RV function should be measured, owing to their prognostic relevance.
- In experienced laboratories, RV strain and/or 3D measurements of RV volumes may be considered to overcome the existing limitations of conventional RV function indices. When available, CMR is the preferred method to assess the RV due to its high accuracy and reproducibility.
- Echocardiographic criteria for grading severity of TR:
- Qualitative: tricuspid valve morphology, color flow regurgitant jet
- Semiquantitative: vena contracta width, proximal isovelocity surface area (PISA) radius, hepatic vein flow, tricuspid inflow
- Quantitative: Effective regurgitant orifice area (EROA), regurgitant volume, enlargement of cardiac chambers/vessels
- Diuretics are useful in the presence of right HF.
- The addition of an aldosterone antagonist may be considered to counterbalance the activation of the renin-angiotensin-aldosterone system associated with hepatic congestion.
- Dedicated treatment of pulmonary HT is indicated in specific cases.
- Although data are limited, rhythm control may help to decrease TR and contain annular dilatation in patients with chronic AF.
- In the absence of advanced RV dysfunction or severe pulmonary hypertension, none of the above-mentioned therapies should delay referral for surgery or transcatheter therapy.
- In patients with signs and symptoms of right-sided HF attributable to severe TR (Stages C and D), diuretics can be useful (Class 2a, Level of evidence C expert opinion).
- In patients with signs and symptoms of right-sided HF attributable to severe secondary TR (Stages C and D), therapies to treat the primary cause of HF (e.g. pulmonary vasodilators to reduce elevated pulmonary artery pressures, guideline-directed medical therapy (GDMT) for HF with reduced LVEF, or rhythm control of AF) can be useful (Class 2a, Level of evidence C expert opinion).
- Relevant TR requires early intervention to avoid secondary damage of the RV.
- TR should be liberally treated at the time of left-sided valve surgery. Isolated surgery of severe secondary TR (with or without previous left-sided valve surgery) requires comprehensive assessment of the underlying disease, pulmonary hemodynamics, and RV function.
- Primary TR:
- Surgery is recommended in patients with severe primary TR undergoing left-sided valve surgery (Class I, Level of evidence C)
- Surgery is recommended in symptomatic patients with isolated severe primary TR without severe RV dysfunction (Class I, Level of evidence C)
- Surgery should be considered in patients with moderate primary TR undergoing left-sided valve surgery (Class IIa, Level of evidence C)
- Surgery should be considered in asymptomatic or mildly symptomatic patients with isolated severe primary TR and RV dilatation who are appropriate for surgery (Class IIa, Level of evidence C)
- Secondary TR:
- Surgery is recommended in patients with severe secondary TR undergoing left-sided valve surgery (Class I, Level of evidence B)
- Surgery should be considered in patients with mild or moderate secondary TR with a dilated annulus (≥40 mm or >21 mm/m2 by 2D echocardiography) undergoing left-sided valve surgery (Class IA, Level of evidence B)
- Surgery should be considered in patients with severe secondary TR (with or without previous left-sided surgery) who are symptomatic or have RV dilatation, in the absence of severe RV or left ventricular dysfunction and severe pulmonary vascular disease/hypertension (Class IIa, Level of evidence B).
- Transcatheter therapy and surgery may be considered in selected cases. A multidisciplinary heart team, including HF specialists, should be considered for assessment and treatment planning.
- Transcatheter techniques have recently emerged as potential treatment options of TR. Preliminary results show improvement in TR severity and symptoms with low complication rates. Further prospective studies are needed to show the prognostic impact of these treatments in HF patients
- For patients with VHD for whom intervention is contemplated, individual risks should be calculated for specific surgical and/or transcatheter procedures, using on-line tools when available, and discussed before the procedure as a part of a shared decision-making process (Class 1, Level of evidence C expert opinion).
- Patients with severe VHD should be evaluated by a multidisciplinary heart valve team when intervention is considered (Class 1, Level of evidence C expert opinion).
- In asymptomatic patients with any type of valve intervention, a baseline postprocedural TTE followed by periodic monitoring with TTE is recommended.
- In patients with severe TR (Stages C and D) undergoing left-sided valve surgery, tricuspid valve surgery is recommended (Class 1, Level of evidence C limited data).
- Transcatheter tricuspid valve intervention TTVIs are under clinical development and early registry and study data have demonstrated their feasibility to reduce TR.
- Transcatheter treatment of symptomatic secondary severe TR may be considered in inoperable patients at a heart valve center with expertise in the treatment of tricuspid valve disease (Class IIb, Level of evidence C).
- Transcatheter therapy and surgery may be considered in selected cases. A multidisciplinary heart team, including HF specialists, should be considered for assessment and treatment planning.
- Transcatheter techniques have recently emerged as potential treatment options of TR. Preliminary results show improvement in TR severity and symptoms with low complication rates. Further prospective studies are needed to show the prognostic impact of these treatments in HF patients
- For patients with VHD for whom intervention is contemplated, individual risks should be calculated for specific surgical and/or transcatheter procedures, using on-line tools when available, and discussed before the procedure as a part of a shared decision-making process (Class 1, Level of evidence C expert opinion).
TV

TAVI in complex anatomies

AI-enabled procedural learning

Case planning for lifetime management

Strategies to reduce conduction disturbances following TAVI

TAVI Summit 2026 - Introduction

Artifical intelligence in structural heart imaging

Anatomy for structural heart therapies

EACTS Symposium 2025
Transcatheter Aortic Valves Implant - 2025

TAVI strategies for patient lifetime management
HUB
Tri.Fr 2 years outcomes
bRIGHT clinical data release | PCR LV 2025
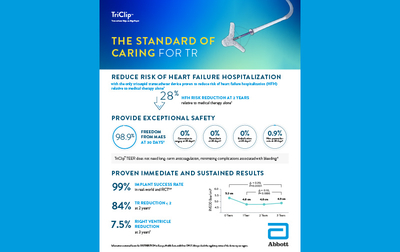
The standard of caring for TR

TEER G5 Brochure 2025
TRILUMINATE Pivotal - 2-year update EuroPCR 25
bRIGHT 2-year real-world outcomes
2-year outcomes from the TRILUMINATE Pivotal trial

bRIGHT study