Heart Failure
STAGES OF HEART FAILURE1,2
CLASS I
No symptoms or limitations to physical activity.
CLASS II
Slight limitations of physical activity. Comfortable at rest; ordinary physical activity results in feeling tired and shortness of breath.
CLASS III
Significant limitations of physical activity. Less than ordinary activity causes results in feeling tired and shortness of breath.
CLASS IV
Unable to carry on any physical activity without discomfort. Tired and shortness of breath even at rest.

INTERMACS PROFILES
- NYHA classification does not offer adequate description to allow optimal selection of patients for current options of medical and device therapies, HTx and MCS
- NYHA III and IV Patients who may be considered for MCS can now be classified using 7 INTERMACS profiles.

MECHANICAL CIRCULATORY SUPPORT (MCS)
Indications for short- and long-term MCS should be based on the INTERMACS profiles4

INTERAGENCY REGISTRY FOR MECHANICALLY ASSISTED CIRCULATORY SUPPORT PROFILE DESCRIPTIONS OF PATIENTS WITH ADVANCED HEART FAILURE4
| Profile | Time frame for intervention |
|---|---|
| Profile 1. Critical cardiogenic shock Patient with life-threatening hypotension despite rapidly escalating inotropic support, critical organ hypoperfusion, often confirmed by worsening acidosis and/or lactate levels.“Crash and burn.” | Definitive intervention needed within hours. |
| Profile 2. Progressive decline Patient with declining function despite i.v. inotropic support, may be manifest by worsening renal function, nutritional depletion, inability to restore volume balance. “Sliding on inotropes.” Also describes declining status in patients unable to tolerate inotropic therapy. | Definitive intervention needed within few days. |
| Profile 3. Stable on inotrope or inotrope-dependent Patient with stable blood pressure, organfunction, nutrition, and symptoms on continuous i.v. inotropic support (or a temporary circulatory support device or both) but demonstrating repeated failure to wean from support due to recurrent symptomatic hypotension or renal dysfunction. “Dependent stability.” | Definitive intervention elective over a period of weeks to few months. |
| Profile 4. Frequent Flyer Patient can be stabilized close to normal volume status but experiences daily symptoms of congestion at rest or during activities of daily living. Doses of diuretics generally fluctuate at very high levels. More intensive management and surveillance strategies should be considered, which may in some cases reveal poor compliance that would compro-mise outcomes with any therapy. Some patients may shuttle between 4 and 5. | Definitive intervention elective over a period of weeks to few months. |
| Profile 5. Housebound Comfortable at rest and with activities of daily living but unable to engage in any other activity, living predominantly within the house. Patients are comfortable at rest without congestive symptoms, but may have underlying refractory elevated volume status, often with renal dysfunction. If underlying nutritional status and organ function are marginal, patients may be more at risk than INTERMACS 4, and require definitive intervention. | Variable urgency, depends upon maintenance of nutrition, organ function, and activity. |
| Profile 6. Exertion limited Patient without evidence of fluid overload, comfortable at rest and with activities of daily living and minor activities outside the home but fatigues after the first few minutes of any meaningful activity. Attribution to cardiac limitation requires careful measurement of peak oxygen consumption, in some cases with haemodynamic monitoring, to confirm severity of cardiac impairment. “Walking wounded.” | Variable, depends upon maintenance of nutrition, organ function, and activity level. |
| Profile 7. Advanced NYHA class III symptoms Patient without current or recent episodes of unstable fluid balance, living comfortably with meaningful activity limited to mild physical exertion. | Heart transplantation or MCS may not be currently indicated. |
| Modifiers for profiles | Possible profiles that can be modified |
| Temporary MCS can modify profile only in hospitalized patients. They include IABP, ECMO, TandemHeart, LVAD, Impella. | 1, 2, 3 |
| Arrhythmia can modify any profile. They include recurrent ventricular tachyarrhythmias that have recently contributed substantially to clinical compromise, frequent ICD shocks or requirement for external defibrillation, usually more than twice weekly. | 1-7 |
| Frequent episodes of HF decompensation characterize patients requiring frequent emergency visits or hospitalizations for diuretics, ultrafiltration, or temporary i.v. vasoactive therapy. Frequent episodes may be considered as at least two emergency visits/admissions in the past 3 months or three in the past 6 months. | 3 if at home, 4, 5, 6. Rarely for profile 7. |
Connext
TV
TV
TV

Anatomy for structural interventions therapies (ASD, PFO, LAAO)

Transcatheter tricuspid valve repair: Cases, tips and tricks

M-TEER: Best treatment strategies for FMR AND DMR

Latest evidence in patient selection for T-TEER
Echo procedural approach for transcatheter tricuspid repair

M-TEER: State of the art echocardiography imaging modalities

EHRA 2026 | Tutorials | PFA/LAAO

TAVI in complex anatomies

AI-enabled procedural learning

Time to move TAVI upstream
HUB
VANTAGE Trial - 1-year clinical outomes
Tri.Fr 2 years outcomes
Navitor 5-years data from CRT
Tendyne expanded clinical study | PCR LV 2025
EXPAND G4 clinical data release | PCR LV 2025
bRIGHT clinical data release | PCR LV 2025
Navitor Active-Sealing Cuff

Navitor Low PPI & Radiopaque Markers
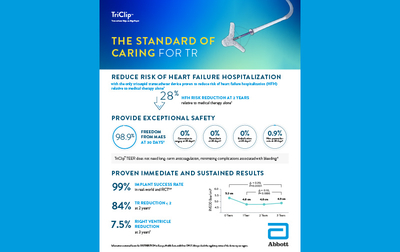
The standard of caring for TR

TEER G5 Brochure 2025
References
- Jessup M, Brozena S. Heart Failure. N Engl J Med. 2003;348(20):2007–2018. doi.org/10.1056/NEJMra021498.
- www.heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure. Accessed July 2023.
- Teuteberg JJ, Cleveland JC, Cowger J, et al. The Society of Thoracic Surgeons Intermacs 2019 Annual Report: The changing landscape of devices and indications. Ann Thorac Surg. 2020;109(3):649–60. doi.org/10.1016/j.athoracsur.2019.12.005.
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi.org/10.1093/eurheartj/ehab368.
- Eisman AS, Shah RV, Dhakal BP, et al. Pulmonary capillary wedge pressure patterns during exercise predict exercise capacity and incident heart failure. Circ Heart Fail. 2018;11(5):e004750. doi.org/10.1161/CIRCHEARTFAILURE.117.004750.
- Mehra MR, Canter CE, Hannan MM, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: a 10-year update. J Heart Lung Transplant. 2016;35(1):1–23. doi.org/10.1016/j.healun.2015.10.023.
- Stevenson LW, Pagani FD, Young JB, et al. INTERMACS profiles of advanced heart failure: the current picture. J Heart Lung Transplant. 2009;28(6):535–541. doi.org/10.1016/j.healun.2009.02.015.