TRICLIP™ TRIKUSPIDALKLAPPENREPARATURTRANSKATHETER
EDGE-TO-EDGE REPARATUR (TEER)
EDGE-TO-EDGE REPARATUR (TEER)
Die TriClip™ Transkatheter Edge-to-Edge Repair (TEER) bietet
eine minimal-invasive Behandlungsoption für Patienten mit
symptomatischer, schwerer Trikuspidalinsuffizienz (TI),
für die eine Operation ein hohes Risiko darstellt.1
EINE HOCHMODERNE BEHANDLUNGSOPTION FÜR PATIENTEN MIT HOHEM OPERATIONSRISIKO
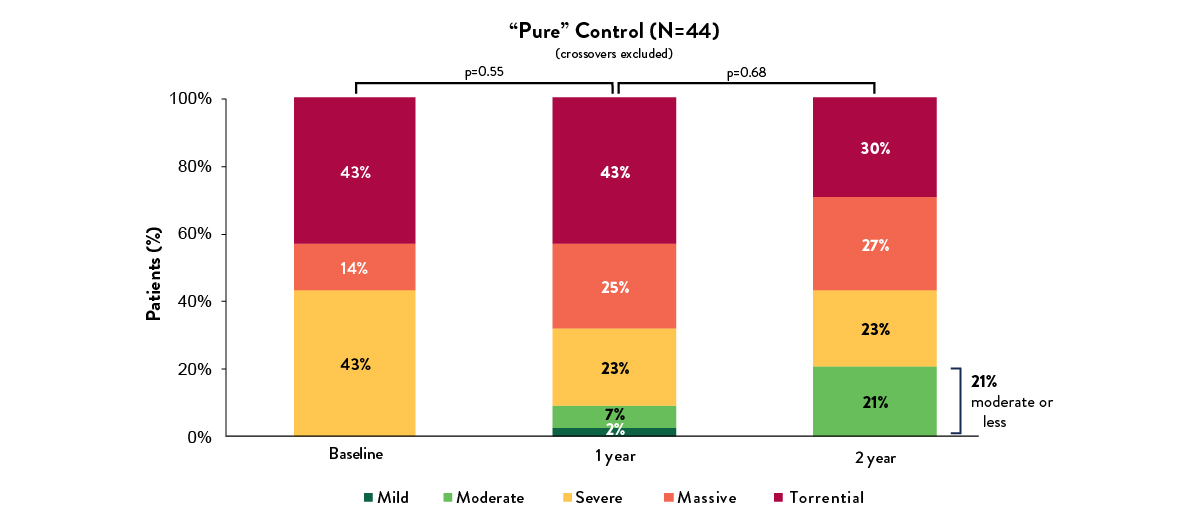
TriClip™ TEER ist eine risikoarme,5 minimal-invasive, nicht-chirurgische Behandlungsoption für symptomatische Patienten mit schwerer Trikuspidalinsuffizienz (TI), bei denen ein hohes Risiko für eine Operation besteht und die durch eine alleinige medikamentöse Therapie keine Besserung erfahren.

TV

What to expect on the AV horizon

AV VALVES Summit 2026 | Wrap-up

Beyond the guidelines - heart team decision-making

Tricuspid Case Parade - optimizing procedural outcomes

Mitral Case Parade - challenging clinical scenarios
Al and Imaging - transforming patient care

Navigating the VHD guidelines and new evidence

AV VALVES Summit 2026 | Introduction
")
HFA 2026 | How to manage a secondary AV valve disease (E.Donal)

HFA 2026 | How to manage a secondary AV valve disease (L.Sanchis)